Latest in Literature: Maropitant as a perioperative analgesic? & Pelvic limb fracture management in psittacines
These brief summaries are designed to be quicker and easier to read than a full journal article, but more informative than an abstract. Basically I want to give you the background of why the study is important, their findings, if there were any major deficiencies in the study, and what you should take away from it in the end. I hope this saves you some time!
Roeder M, Boscan P, Rao S, et al. Use of maropitant for pain management in domestic rabbits (Oryctolagus cuniculus) undergoing elective orchiectomy or ovariohysterectomy. Journal of Exotic Pet Medicine 2023;47:14–20.
Introduction:
Maropitant is an neurokinin-1 (NK1) receptor antagonist. These receptors are found in the vomiting center of the brain, as well as many peripheral tissues, including throughout the gastrointestinal tract. Maropitant has been found to have inhalant anesthetic MAC-sparing effects in dogs, cats and rats, but no studies have shown the benefits of using maropitant as a perioperative analgesic. There have been 2 pharmacokinetic studies looking at maropitant in rabbits, but no pharmacodynamic studies prior to this study.
Methods:
This prospective study across 3 institutions looked at healthy rabbits presenting for elective altering. A total of 28 female and 23 male rabbits were included; there were 17 rabbits in the 2 mg/kg maropitant group, 19 rabbits in the 10 mg/kg maropitant group, and 15 rabbits in the saline control group. 2 mg/kg is the canine label dose and a previous pharmacokinetic study in rabbits showed that a 10 mg/kg SQ dose resulted in plasma concentrations that were shown to be effective in dogs. Any rabbits that had anesthetic and/or surgical complications were excluded from the study. A variety of anesthetic protocols were used, but rabbits were always administered buprenorphine 0.06 mg/kg IM q8hrs and meloxicam 1 mg/kg IM q24hrs for analgesia. Surgeons and observers were blinded to which rabbits were in each group.
Rabbits were monitored post-operatively using a continuously recording video camera for 24 hours or until discharge. Clips of the footage taken at regular intervals were viewed by multiple blinded observers to assess pain, behavior and activity scores. The rabbit facial grimace scale and a pain related behavioral assessment scale were used to score the rabbits. Food intake and fecal output were also measured post-operatively.
Results/Discussion:
Food intake and fecal output decreased somewhat in the rabbits that received the higher dose of maropitant, but the authors noted a larger sample size is needed to confirm the effect of the drug and dosage on the rabbit GI tract. Interestingly, male and female rabbits showed comparable pain and behavior scores, despite the likely variation in soft tissue trauma and surgical time.
Potential factors that could have affected the outcome of this study included variation in anesthetic protocols, surgeon experience levels (varying degree of visceral pain and soft tissue trauma secondary to technique), small sample size, and the fact that many rabbits were discharged earlier than 12 hours so the authors were unable to include and assess that data, which in turn could have skewed food intake/fecal output data.
The authors recommend against using maropitant 10 mg/kg SQ due to potential negative effects on the gastrointestinal tract. Ultimately, larger studies are needed to determine if maropitant is an effective visceral pain analgesic in rabbits.
Takeaways:
While many of us have seen anecdotal evidence of maropitant helping with what we presume to be visceral pain (with GI stasis, liver lobe torsion, etc), Maropitant 2 mg/kg and 10 mg/kg SQ did not reduce pain in rabbits undergoing elective orchiectomy or ovariohysterectomy compared to control groups in this study. Is it possible we are seeing improvement in the aforementioned cases because the maropitant is addressing nausea rather than pain? Ultimately, we need more studies to further assess this. Given the lack of adverse effects with administration of 2 mg/kg, administration of this dosage may not help, but is unlikely to hurt.
Hollwarth AJ, Dutton TAG. Retrospective Analysis of Pelvic Limb Fracture Management in Companion Psittacine Birds (60 Cases). Journal of Avian Medicine and Surgery 2023;37(2): 165-174.
Introduction:
While psittacine pelvic limb fractures are common, there is limited literature regarding fracture management, healing times and complication rates. This paper hypothesized that birds undergoing surgical fracture repair would heal more quickly and have lower complication rates.
This is a retrospective cross sectional study evaluating pelvic limb long bone fractures in companion psittacines from 2005 to 2020. If you’ve long forgotten study classifications like I have - this means the study assessed medical records from a set time period and gathered data to evaluate the prevalence of the problem (pelvic limb fractures) and characteristics about those affected (type/location of fracture, treatment elected, time to healing, complications, etc). This type of study is unable to determine cause-and-effect relationships, but can make inferences about correlations or gather data to support further research.
Methods:
This study included 60 cases consisting of 22 different species, aged 8 weeks to 25 years old, equally distributed between male and female (among sexed birds). 71.7% of fractures were tibiotarsal, with femoral then tarsometatarsal following, fairly evenly split. The most common fracture types were closed, simple and diaphyseal fractures. Methods used for fracture management included external coaptation, surgery and cage rest.
A variety of fracture management methods were used, with surgical correction most commonly used for the tibiotarsus, and medical and surgical options used nearly equally for femoral fractures and tarsometatarsal fractures.
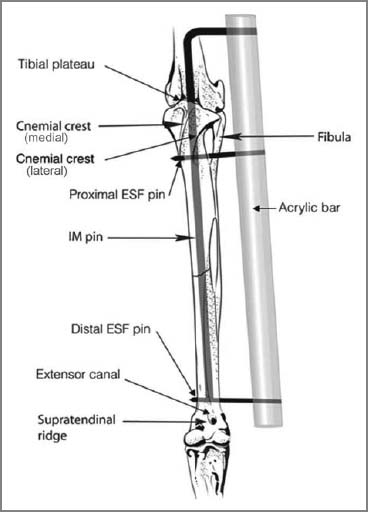
Diagram illustrating ESF-IM tie-in fixator used in a tibiotarsal fracture of a raptor, From: Bueno I, Redig PT, Rendahl AK. External skeletal fixator intramedullary pin tie-in for the repair of tibiotarsal fractures in raptors: 37 cases (1995–2011). JAVMA 2015;247:1154–1160.
The study defined satisfactory resolution of repair as a palpable firm swelling and stability of bone on palpation or visible callus on radiographs, as well as return to normal function in the affected limb.
Complications observed included postoperative discomfort, patient interference, bandage complications such as swelling, or wounds, osteomyelitis, refracture or fracture of other long bones, delayed healing or death secondary to fracture complications or during anesthesia/surgery for fixation. 25 out of 60 cases reported 1 or more complications, and there was no significant difference in complication incidence between the fracture locations. Utilizing an aluminum foam-backed splint/soft tissue bandage had the highest complication rate at 61.5% of cases and tape splints had a complication rate of about 41%. Surgical pinning alone had a complication rate of about 35%.
Documented reasons for avoiding surgical pinning included open fractures with gross contamination, temporary splinting to determine viability of the foot, poor bone density, cost of procedure, size of the patient and a final case consisting of only a chip fracture which could not be stabilized surgically.
Complications led to amputation of the affected limb in 3 cases. Birds that died during healing all had comorbidities including metabolic bone disease, an episode of aspiration during medication administration and psittacosis.
Results/Discussion:
Average time to healing was 33 days. Resolution was obtained in 47/55 (86%) of patients that were followed to conclusion, however there were complications in 25/60 or nearly 42% of patients. The most common complication was patient interference with bandages and/or splints, and it occurred most commonly with external coaptation.
47 of the cases were followed during healing and healing times ranged from 11 to 121 days, with an average of 33 days. Femoral fractures healed quicker and tibiotarsal fractures required the longest time to heal on average, but they all had similar median healing time of about 31 days. Birds less than 490 grams had faster average and median time to callus versus larger patients. Birds that experienced complications had longer average and median healing times.
Delayed union was observed in 4 cases, with osteomyelitis and attempted conservative management techniques apparent contributing factors.
46 out of 50 patients followed long term had no reported complications. The 4 birds that developed long term complications included mild angular limb deformities, pododermatitis in the contralateral foot and digit arthrosis, all of which were either non-issues for the patient or were able to be treated medically.
The authors note that ultimately, fracture management should be determined on a case-by-case basis. Splinting and bandaging are most commonly used in small birds <300g. Tape splinting was very commonly reported, but also had a higher complication rate than reported in a previous study, which should be taken into account when determining fixation method.
External coaptation resulted in a much higher complication rate than surgical intervention, likely due to the behavior of psittacins. Ensuring appropriate analgesia and judicious use of an elizabethan collar can help prevent patient interference.
Study limitations included the retrospective nature, small sample sizes and subjective assessment of healing by 10 different practitioners. Further studies comparing patients with and without comorbidities could be helpful.
Takeaways:
There is no one correct way to repair a pelvic limb fracture in a psittacine because the best treatment will depend on the patient in front of you, the client’s finances, and your comfort level with different repairs. However, if possible, surgical repair with an external skeletal fixator - intramedullary tie-in fixator results in a quicker resolution with a lower complication rate, especially in larger psittacines.
Do you agree with my assessment of these studies? Do you have questions that I didn't answer? Comment below or reach out to me!