How to perform a COMPLETE rabbit physical exam

I’m going to start out this clinical series by going back to the basics. Even if you’ve been seeing rabbits for years, read on for a review of performing a complete, systematic physical exam on rabbits.
You probably heard this in vet school, but the most important factor in performing a complete physical exam, every time, in any species, is to develop a system. In my first few months as a veterinarian, I developed a system for my physical exam in cats and dogs, which is not altogether unique, taking a nose to tail approach. Since most of our exotic companion mammals are prey species, I have adapted that technique to try to minimize fear and anxiety in these patients. Rabbits also have some unique anatomic characteristics that should be kept in mind when performing a physical exam.
Before I ever touch the patient, I perform an observational exam. If the rabbit is in an exam room, I will have the owner open the carrier before I come in the room, lay out a non-slip mat out and encourage the rabbit to move around. If I am examining the patient as a drop off or hospitalization, I will visually examine them in the kennel prior to handling.
A few things I look for:
respiratory rate and character
ocular and/or nasal discharge
mobility (any limping, dragging limbs, etc)
signs of pain such as squinted eyes, flared nostrils and pinned back ears (see this graphic of the Rabbit Grimace Scale)
body condition (we will revisit this on the hands-on exam as well)
visible changes to the coat and skin.
Sometimes, rabbits will be too stressed to come out on their own, or will attempt to flee when removing them from the carrier or kennel. In these cases, it may be prudent to administer a mild sedative. Oral options are gabapentin and trazodone if ample time is available, or if injectable is indicated, butorphanol and/or midazolam administered IM is typically adequate. If I observe dyspnea, I will often administer a light dose of midazolam and place the patient in oxygen in a quiet area for 20-30 minutes before I attempt a full exam.

Inquisitive, comfortable rabbit (ears perked, eyes wide open)
After the observational exam, I start my physical exam with the pet facing away from me, often with the head tucked in a towel or between my assistant’s arm and body in a football hold. I auscult both the heart and lungs, sometimes lifting them slightly off the table if heart sounds are muffled in the initial position, and then move on to the abdomen. Our small mammal friends are like horses and ruminants - we need to listen for gastrointestinal borborygmi. I like to listen in each ‘quadrant’ of the abdominal cavity and you should be able to hear a gurgle every 15-30 seconds. Stress can reduce GI sounds, so if the rabbit appears otherwise normal on physical exam, a slight reduction may not be a concern as long as the rabbit is eating and defecating regularly. This will become easier the more physical exams you do - you have to know ‘normal’ to know abnormal, and after awhile you will be able to easily detect hypo- and hyper-motility.

This rabbit wanted to stretch out and was a 'less-is-more' rabbit when it comes to restraint. However, if it is an unfamiliar rabbit, make sure your assistant has adequate control to prevent the rabbit from jumping or lunging by placing their hands in front of/on top of each shoulder blade.
While the rabbit is still facing away from me, I begin my palpation by gently running my hands over the rabbit's body to assess body condition, palpate in the fur for any skin lesions or masses and palpate the lymph nodes. After palpating along the superficial thorax and abdomen, I progress to palpating along the mandible and ventral neck, palpating for any lymph node enlargement and swellings along the mandible. I check the compliance of the thoracic cavity by gently compressing the sternum - if there is concern for decreased compliance, I will have the assistant turn the rabbit’s head towards me and gently tilt the front of the rabbit toward the ground to check for positional exophthalmos.
Abdominal palpation should reveal a soft, malleable stomach, typically not extending beyond the rib cage, and a large, pliable cecum taking up the majority of the abdominal cavity. Borborygmi can often be appreciated when running the intestinal contents and cecum through your fingers. The liver is often not palpable due to the predominance of the GI tract and should not extend beyond the margins of the rib cage. The kidneys are present along the dorsal body wall on either side of the spine, with the right kidney typically located more cranially. They are somewhat more mobile than our small animal counterparts. If the cecum is prominent, it may not always be possible to feel both kidneys. The urinary bladder can be felt in the central caudal abdomen and should be cautiously palpated as cases of rupture on rough palpation have been documented. It can be normal for a small amount of calcium salts, or bladder sludge, to be palpable in the ventral bladder or visible on expression.
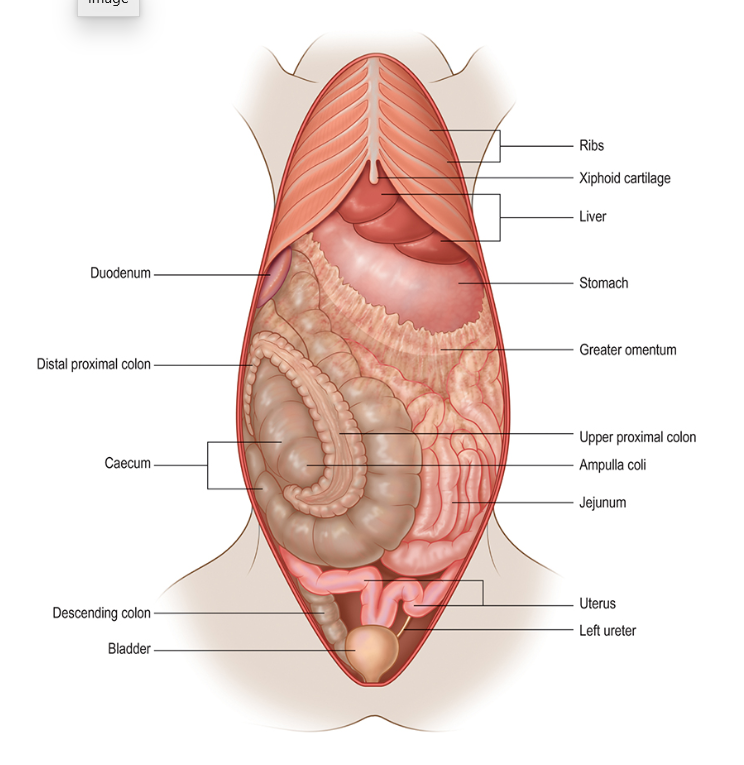
Abdominal cavity anatomy and orientation, from: Varga Smith M ed. Textbook of Rabbit Medicine. 3rd ed. Poland: Elsevier Limited; 2023.
In females, the uterus and ovaries are typically not palpable unless enlarged. However, uterine neoplasia is so common in rabbits over a year of age, it is often appreciated in entire females. After abdominal palpation, I lift the tail to examine the rectal mucosa and take a rectal temperature. The rectal mucosa is very friable so exercise caution.
Then I like to check each limb for normal range of motion and for any crepitus/clicking at each joint. Make sure your assistant is supporting the front end of the rabbit when examining the rear limbs - many rabbits try to move forward when taking their rear limbs through range of motion.
With the assistant holding the rabbit against their body with one hand supporting the thorax and the other supporting the hindquarters, the ventral surface of the rabbit can be examined.

Assistant restraint with one hand supporting hindquarters and other supporting thorax. Note that this rabbit is extremely overweight.
Intact males should have a visible scrotal sac on either side of the caudally located penis on the caudoventral pelvis. Testicles should descend by about 12 weeks of age, however, rabbits have open inguinal canals and many rabbits can retract their testicles abdominally when stressed. If intact males have retracted their testicles, they can often be gently massaged caudally into the scrotal sacs utilizing gravity. Cryptorchidism is uncommon, but it does happen! If you can’t manipulate the testicles into the scrotal sac, it is possible that you will be able to once the animal is under sedation, and if not - you may have a true cryptorchid patient!
Males neutered at a young age often have minimal scrotal sac development but can be easily sexed by gently extruding the penis. The rabbit penis has a round opening while the vulva is a linear orifice.

Comparing a female to a neutered adult male.
Mature intact females often have a rather prominent vulva and mammary glands can typically be appreciated on either side of the ventral abdomen. They also typically develop a large dewlap; if a female is spayed later in life, it may never fully regress. Males do have nipples, but they are typically not appreciable unless searched for.

Intact female rabbit with a large dewlap
While the rabbit is held in this position I check for perineal soiling (urine staining, clumped fecal material or cecotrophs in fur) and examine the scent glands on either side of the genitals for impaction or infection. There is often a small amount of odorous brown or yellow waxy debris built up in each fold of skin. This can be gently cleaned out with moistened cotton-tipped applicators.
Then I examine the palmar and plantar surfaces of each limb. The plantar surface of each hindlimb may have a narrow hairless tract - this can be totally normal, but make sure there are no crusts, swellings or open wounds present. Check each digit for swelling/discharge/redness around the nail base, abnormal nail growth or abnormal range of motion.
I also examine the medial aspect of the forelimbs for any crusts or discharge. Rabbits groom their face with their front paws, so they will often build up discharge in this location if they are still grooming regularly. I sometimes see this even if they don’t have nasal discharge as the first sign of upper respiratory issues.

Young rabbit with nasal discharge, discharge on medial forelimbs and soiled perineum.
Lastly, I have the assistant place the rabbit back on the non-slip mat with the head towards me and I examine the face and oral cavity. The face should be free of discharge and appear symmetrical. I gently palpate along the cheeks feeling for any swellings or cheek teeth spurs, along the zygomatic arch and around the base of the ears. I check for pupillary light and dazzle reflexes. Direct PLR is much more reliable than consensual in rabbits, but is often slower and weaker than what we are used to in other small animals.
I use an ophthalmoscope to evaluate internal ocular structures. It is fairly common for older rabbits to have immature cataracts or lenticular sclerosis; rabbits affected by Encephalitozoon cuniculi in utero can develop cataracts with subsequent phacoclastic uveitis at any age.
I use an otoscope with the largest cone that the ear canal will comfortably accommodate to visualize the outer ear canal. It is common for lop eared rabbits to have a moderate amount of white to pale yellow waxy exudate that can resemble purulent debris. You can determine which you are dealing with by examining microscopically. Wax will have minimum cellularity and bacteria, while purulent exudate is often rampant with bacteria and heterophils. I can often very carefully visualize the eardrum in non-lop eared rabbits by gently grasping the ear near the base and using gentle pressure to straighten the bend in the canal, however, it is nearly impossible in lops due to the bend in their ear canals. If the rabbit seems uncomfortable at all, I discontinue and proceed with sedation if a full otic exam is indicated.
Thick, proliferative crusts are sometimes present, indicating likely Psoroptes cuniculi infection. If the canal is not obstructed, I can often see mites moving in the canal using the otoscope. If confirmation is needed, you can use a dry cotton tipped applicator or remove a small flake of the crusts (try not to remove directly from skin as it is very painful!) and examine the debris microscopically with a small amount of mineral oil.

Rabbit with severe Psoroptes infestation affecting both ears and the facial/neck skin
The oral exam consists of much more than just a visual exam. I start by gently moving the lower jaw laterally back and forth relative to the remainder of the skull to evaluate cheek teeth occlusion. The teeth should slide back and forth without catching. I also move the jaw vertically and slightly front-to-back to ensure appropriate range of motion of the temporomandibular joint. I lift the lips and visually examine the occlusal surface of the incisors from the rostral aspect and lateral aspect. The upper incisors have a beveled edge where they occlude with the lower incisors at a 45 degree angle. A pair of small peg teeth are located behind both upper and lower incisors. At rest the lower incisors should sit between the caudal upper incisors and upper peg teeth. I check the skin around the mouth for salivary staining or facial fold erythema.

Normal length and occlusion of upper and lower incisors
An abbreviated oral exam can be performed on most animals, but sedation or full anesthesia is indicated for a full oral exam. Otoscopes with a plastic cone have been used historically, but if you are going to see exotics regularly I highly recommend investing in a bi-valve nasal/oral speculum. These provide a much wider range of view when utilized. I make sure my assistant has adequate restraint and then use my left hand to gently stabilize the head. With my right (dominant) hand, I place the speculum in the diastema and gently open it. In small rabbits, you can often view all four dental arcades at once, but in larger rabbits I will often look at one side at a time.

Utilizing a bi-valve nasal speculum to examine the cheek teeth of a rabbit (Note that this rabbit's left lower cheek have been previously extracted and the upper cheek teeth are longer than they would be with normal apposing teeth)
The cheek teeth should have a slight angle to the occlusal surface with the ventral cheek teeth appearing longer lingually and slanting to a shorter edge buccally. The maxillary cheek teeth reflect the reverse. This should not be mistaken for cheek teeth spurs or points. The cheek teeth appear somewhat uniform but in older rabbits may display some darkening in the folds of the teeth. The length of the dental crowns should be symmetrical from side to side. The presence of swelling, abrasions, blood, a foul odor or purulent discharge is abnormal. If dental disease is suspected, the rabbit should be sedated or anesthetized for a complete oral exam and skull and dental radiographs or computed tomography.

Graphical depiction of rabbit cheek teeth occlusion, note the slight angle of occlusion and appearance of small mandibular lingual spurs and maxillary buccal spurs. From: Quesenberry K, Orcutt CJ, Mans C, et al. eds. Ferrets, Rabbits, and Rodents: Clinical Medicine and Surgery. 4th ed. St Louis: Elsevier, Inc; 2021.
I hope this helps you perform more thorough rabbit physical exams! Let me know in the comments if you have any feedback, questions, or a topic for a future post.
A special thanks to Sarah Cox, DVM for contributing photos for this post.